Labor costs and low morale are looming emergencies for medical systems revenue cycle directors in 2022. Doctors and nurses are suffering burnout and quitting or reducing hours. These medical staff shortages in turn drive up employment costs when hospitals increasingly rely on temporary staff like traveling nurses. Revenue cycle directors must proactively address the issue to protect patient care and prevent hospital insolvency.
Nurse shortages were common before the pandemic. But COVID has worsened the situation.
After two years of watching unvaccinated COVID patients die and experiencing workplace violence, nurses are quitting in droves.
Over 500,000 nurses are expected to leave the field this year (Neisloss, Liz. ‘Travel nurse salaries driven up in the pandemic, creating ‘unsustainable’ hospital costs.’ GBH Boston Public Radio. Feb. 3, 2022).
Over one-third of all nurses—34 percent—plan on quitting in the next year, according to one industry report. Burnout, stressful environments and inadequate compensation are the main reasons for wanting to leave their jobs. The U.S. will have a shortage of 1.1 million nurses by the end of 2022.
This trend of clinical staff shortage might be part of the post-COVID “Great Resignation,” which affected almost every industry.
But employment analysts note healthcare’s unique level of stress during the pandemic. Unvaccinated patients and their families sometimes react angrily at their diagnoses, threatening or assaulting staff.
It’s not surprising many staff nurses are fed up with their working conditions. So they are resigning but opting to work as traveling nurses, who can earn $10,000 a week. That’s a “life-changing sum,” said one, in a National Public Radio story.
When nurses quit their jobs to work for a traveling nurse agency, this creates staff shortages at institutions they left.
The result is hospitals have had to rely increasingly on temporary staff. The labor shortage means traveling nurses often make $120-$200 an hour. Travel nurse agencies often tack on an additional 50 percent (Neisloss).
Temporary staff’s higher salaries create resentment among permanent employees, who train visiting nurses but make a fraction of their wages. Clearly this is unsustainable for many hospitals, both in terms of morale and costs. And it may push them over the edge financially.
“As this shortage has worsened and COVID-19 hospitalizations have reached record levels, labor costs for hospitals have increased dramatically,” the American Hospital Association warned in January. “This is occurring at a time when many hospitals and health systems are still facing other immense financial constraints. For many hospitals around the country this has led to an unsustainable situation that threatens their ability to care for the patients and communities they serve.”

Why are clinical staff experiencing burnout?
Nurses, doctors and other frontline staff have worked longer hours on the same pay. They have done so while watching COVID patients suffer and die, many of them needlessly because they were unvaccinated. This subset of patients and their families has been uncooperative to the point of violence.
Assaults on healthcare workers account for 73 percent of non-fatal workplace violence (U.S. Bureau of Labor Statistics, 2018).
Workplace violence
In 2019, registered nurses experienced more than three times the rate of nonfatal workplace violence-related injuries, compared with other occupations.
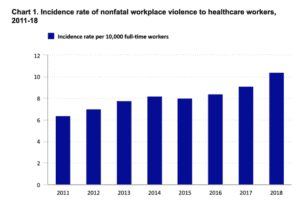
In some hospitals, patient violence against providers has tripled under COVID. It’s hard to reconcile violence against nurses with how much they’re trusted. Americans have rated nursing more ethical than any other profession for 20 years in a row.
Other factors
During this period of nurse shortage, the COVID-19 pandemic has clogged the education pipeline. COVID restrictions have reduced nursing schools’ limited capacity to graduate students. The increase in retiring nurses also means fewer nursing teachers.
Some healthcare organizations have responded to nurse burnout by offering “staff-directed remedies.” These programs can include counseling or support for continuing education. Management says this will fight burnout.
But clinical associations say this is inadequate. One nurse interviewed complained that management’s approach to staff burnout is superficial and lacks commitment. Rather than pay veteran staff nurses more, reduce their overtime or ask them how to improve workplace safety, her hospital had a pizza party. (Kaiser Health News and Nashville Public Radio.)
Action is needed
Health systems have to do more. At the top of the list is hiring and retaining enough nurses to reduce reliance on temporary staff or clinician overtime. The issue of workplace safety is also important. The AHA backs legislation to give healthcare workers the same safety rights as flight crews and airport workers under federal law. And support for this legislation from healthcare systems is important.
Addressing nurses labor costs and morale will thus require creative thinking from hospital financial management, as staffing already consumes 50 percent of most healthcare institutions’ budgets.

Digital healthcare’s toll on doctors and patients
Doctors’ reasons for wanting to leave medicine or reduce hours differ from nurses’.
The increasing amount of time doctors spend on computers inputting test results and other clinical data is one of the primary causes of physician burnout. Physicians know their electronic health records (EHR) system is important. More complete medical histories and other patient data can theoretically result in better care. But physicians resent the amount of time required to maintain the EHR platform.
Initially, the transition to digital healthcare promised improved patient outcomes and hospital profitability. But its impact on providers has been mixed at best, observes a leading healthcare analyst. According to Atul Gawande, an American surgeon and Harvard professor, EHRs have yet to deliver on their early promise.
Gawande grew up programming his own computer. So he represents the kind of physician best equipped to face the challenge of digital transition. Initially he was optimistic about the growing role of EHRs in healthcare. But his own experience with digital transition tempered that initial enthusiasm.
In a 2018 New Yorker article, Gawande describes participating in Partners HealthCare’s $1.6 billion EHR conversion to the Epic platform. Over 18,000 Partners staff spread over twelve hospitals and hundreds of clinics also had to learn to use it.
Although some medical providers saw the benefits, for most the experience simply made them work longer hours performing data input. “Providers don’t go to medical school to become coders,” he observed.
Physicians spent about two hours doing computer work for every hour spent face to face with a patient, according to a 2016 study. In the examination room, physicians devote half of their patient time facing computer screens servicing their EHRs.
These tasks also stretch their days to unsustainable lengths. The University of Wisconsin found that the average workday for family physicians has grown to eleven and a half hours. (Gawande, 2018.)
“The result,” according to Gawande, “has been epidemic levels of burnout among clinicians. Forty per cent screen positive for depression, and seven per cent report suicidal thinking—almost double the rate of the general working population.” (Gawande, 2018.)
But some doctors are more hopeful. Gawande also describes one physician who successfully customized the Epic platform to better serve his surgical unit’s workflow.
In another instance, Gawande describes the use of “medical scribes” who take notes for physicians while they meet with patients.
Although this creates additional staffing expenses, it frees up the physician to focus on the patient. This can theoretically make physicians more efficient and improve patient care.
In the future, native language Artificial Intelligence applications should make this more feasible. Although using a scribe or an AI assistant will mean the physician still has to check their work, this method may reduce strain on physicians. However, this depends on management doing more than simply increasing patient load on doctors.
Regardless of the solution, hospital management needs to be proactive at preventing its staff shortage problem from getting worse. One in five doctors is seriously considering leaving medicine in the next two years. That figure is based on a survey of 20,000 physicians conducted across 124 hospitals.
Burnout, workload, fear of infection, anxiety or depression due to COVID-19, and the number of years in practice are the major causes in staff reducing hours or quitting. (’COVID-Related Stress and Work Intentions in a Sample of U.S. Health Care Workers.’ Mayo Clinic Proceedings: Innovation, Quality & Outcomes. https://www.ama-assn.org/practice-management/physician-health/medicine-s-great-resignation-1-5-doctors-plan-exit-2-years.)

“Our study demonstrates that the U.S. healthcare workforce is in peril,”
says Christine Sinsky, the American Medical Association’s vice president of professional satisfaction. “If even one-third to one-half of nurses and physicians carry out their expressed intentions to cut back or leave, we won’t have enough staff to meet the needs of patients.”So what is the solution to medical staff burnout?
One of the simplest ways to begin solving the clinical labor crisis in healthcare is to start by communicating with staff. Because each hospital or medical system is unique, so are its staffing issues.
Management should also conduct a realistic gut-check about staff turnover costs, patient care and their organization’s financial health. COVID and the digitization of healthcare have placed unparalleled pressure on our medical system. But this creates opportunities as well.
Some medical system managers are waking up to the fact that they benefit from good staff morale. They are paying retention bonuses to keep staff nurses, as well as helping with student loan forgiveness and tuition assistance.
Research clearly shows what will make physicians happier: reducing the amount of time they waste on servicing their EHRs. Chief complaints are that some system users send too many alerts and permission requests or to add notes so long and numerous they are unreadable.
As a consequence, medical “alerts” have multiplied to the point of being ignored.
“Why are nearly all notes in Epic [a major EMR platform]…basically useless to understand what’s happening to a patient during a hospital course?” a Mass General doctor complained on social media.
“Because notes are used to bill, determine level of service and document it rather than their intended purpose, which was to convey our observations, assessments, and plan,” another doctor replied to his post.
“The EMR (electronic medical record) has become mostly fluff with no substance,” another doctor responded. “It exists for billing and coding—not for patient care.” (Koopman et al. “When data drive health: an archaeology of medical records technology.” BioSocieties. Sept. 6, 2021.)
The result is physician burnout due to alert and note fatigue. Drug alerts and diagnostic tests are getting lost in the system.
One study estimated poor EHR design resulted in one-third of drug interactions kept from being prevented. Another study estimates clinical staff override prescription alerts 91 percent of the time anyway. (Weingart et al. https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/1108535.)
Epic and other EHR systems are now promising development of more streamlined systems with a higher user experience. EHR consultants suggest suppressing minor alerts in the development of new digital platforms.

AHA calls for reform
The American Hospital Association recommends that Congress and the Administration increase regulatory scrutiny of health staffing agencies for anticompetitive behavior. (https://www.aha.org/lettercomment/2021-02-04-aha-urges-ftc-examine-anticompetitive-behavior-nurse-staffing-agencies-and)
The AHA also called for an end to health insurers’ burdensome practices of constantly requiring excessive permissions and documentation. This administrative load just adds to provider burnout and diverts staff away from patient care.
Financial breathing room
Revenue cycle managers can play a big role in ensuring the financial health of their organizations with creative financial leadership.
This is where our company, ERISA Recovery, can help.
We are the industry leaders for collecting aged and complex claims that insurance companies owe patients and hospitals.
For over a dozen years, we’ve pioneered the use of Artificial Intelligence (AI) in claims recovery. We can collect old debt when other vendors cannot. And we do it without upfront costs or changing your central billing office’s daily work routine.
Our approach is to leverage a little known but powerful federal law, the Employment Retirement Income Security Act (ERISA). Empowered by our machine learning and the industry’s best analysts, we use this legislation to collect claims up to a decade old.
So if your clinical staff are suffering burnout, contact us today for a free consultation. We can provide financial breathing room for medical organizations hemorrhaging staff costs and suffering low morale.
3030 Lyndon B Johnson Fwy #900 Dallas, TX 75234
Notes:
American Hospital Association. “AHA Urges FTC to Examine Anticompetitive Behavior by Nurse-Staffing Agencies and Commercial Insurers.” (https://www.aha.org/lettercomment/2021-02-04-aha-urges-ftc-examine-anticompetitive-behavior-nurse-staffing-agencies-and)
Farmer, Blake. “Worn-out nurses hit the road for better pay, stressing hospital budgets — and morale.” Kaiser Health News and Nashville Public Radio. (https://knpr.org/npr/2021-10/worn-out-nurses-hit-road-better-pay-stressing-hospital-budgets-and-morale.)
Reinhart, RJ. “Nurses Continue to Rate Highest in Honesty, Ethics.” Gallup polling. (https://news.gallup.com/poll/274673/nurses-continue-rate-highest-honesty-ethics.aspx.)
Gardner, Rebeka L.; Cooper, Emily; Haskell, Jacqueline; Harris, Daniel A.; Poplau, Sara; Kroth, Philip J and Linzer, Mark. “Physician stress and burnout: the impact of health information technology.”
Gawande, Atu. November 5, 2018. “Why Doctors Hate Their Computers.” The New Yorker magazine.
Incredible Health. “Nursing in the Time of COVID-19.” https://www.incrediblehealth.com/wp-content/uploads/2022/03/IH-COVID-19-2022-Summary.pdf.
National Nurses United. November 2021. Workplace Violence and Covid-19 in Health Care How the Hospital Industry Created an Occupational Syndemic. https://www.nationalnursesunited.org/sites/default/files/nnu/documents/1121_WPV_HS_Survey_Report_FINAL.pdf .
Neisloss, Liz. ‘Travel nurse salaries driven up in the pandemic, creating ‘unsustainable’ hospital costs.’ GBH Boston Public Radio. Feb. 3, 2022.
Sinsky, Christine. Mayo Clinic Proceedings: Innovation, Quality & Outcomes, “COVID-Related Stress and Work Intentions in a Sample of U.S. Health Care Workers.”
Weingart, Saul N., MD, PhD; Simchowitz, Brett, BA; Harper Padolsky, MD; et al. Sept. 12, 2009. “An Empirical Model to Estimate the Potential Impact of Medication Safety Alerts on Patient Safety, Health Care Utilization, and Cost in Ambulatory Care.” Archives of Internal Medicine. 2009;169(16):1465-1473. doi:10.1001/archinternmed.2009.252. (https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/1108535.)