ERISA Recovery: EMR and EHR Conversion Specialists
One of the most daunting challenges medical practices face is when they change systems for managing patients’ data during an electronic medical record (EMR) conversion.
If the EMR conversion is less than perfect, hospitals face big potential problems. Technical concerns include protecting cybersecurity, patient confidentiality, and compliance with the Health Insurance Portability and Accountability Act (HIPAA).
But patient care and user experience can also suffer if the EMR conversion loses data important for diagnosis and treatment or for recovering insurance claims. Patients can miss appointments. Lab test notifications and medication alerts can fall through the cracks. The medical practice could lose HIPAA accrediting. Staff workloads increase. Doctors and nurses feel burnt out. And insurance claims go unpaid. In this kind of situation, medical practices can lose millions and patients suffer.
Our company, ERISA Recovery, can help ensure electronic medical record conversion goes smoothly. We are EMR and EHR (Electronic Health records) conversion specialists. We’ve been fine-tuning data mining and machine learning in healthcare payments for over twelve years. We are also the industry experts in the ERISA appeals process.
Who is ERISA Recovery?
Congress passed the Employee Retirement Income Security Act (ERISA) of 1974 to protect workers’ pension and healthcare plans. Because this legislation is federal, it trumps state insurance regulation– as well as many arbitrary insurance claims deadlines.
We use this law, empowered by artificial intelligence and the industry’s best analysts, to recover money insurance companies owe patients and hospitals. We can recover debt from claims up to a decade old.
ERISA Recovery and EMR conversion
If your hospital or medical system is considering EMR or EHR data abstraction and conversion, contact us first. We provide a wide range of EMR and EHR data conversion services.
We’ll help ensure the transfer doesn’t lose data you need to treat patients and collect claims payments.
We provide these services without requiring upfront payment or changing your central billing office’s normal work procedures.
We recently saved a hospital $1.8 million that would have been lost when another vendor failed to transfer legacy data to their updated platform. Our EMR and EHR conversion health IT specialists have over ten years of experience working with all the major systems, including Epic and Cerner EMR conversion jobs.
What is an EMR or EHR conversion?
An EMR conversion is when a medical system changes or updates its patient records into electronic formats. Conversion can mean aggregating all paper documents, clinical notes, test results, prescriptions and medical charts and converting them into digital form. If the data is only for one system, this is an EMR.
But if the platform updates its data system from an EMR to a more comprehensive and universal format, that is an electronic health record (EHR) conversion. The key to remembering the difference is that an EMR is a more focussed medical record specific to one system, but an EHR concerns the patient’s overall health. In the best case scenario, big data sets, artificial intelligence and machine learning will be able to diagnose and treat health problems earlier and more successfully. In the current move to value-based healthcare delivery, many hospitals are trying to turn their EHRs into customized health plans for their patients that deliver the highest possible user experience from diagnosis to treatment to payment.
EHRs can contain all records of patient treatment from one medical system to another. EHR conversions that produce a comprehensive, reliable and universal platform can save hospitals millions. And more importantly, this improves patient experience and recovery.
As of 2017, nearly 9 in 10 (86%) of office-based physicians had adopted any EHR system], and nearly 4 in 5 (80%) had adopted a certified EHR. Since 2008, office-based physician adoption of any EHRs has more than doubled, from 42% to 86%. ONC and the CDC began tracking adoption of certified EHRs by office-based physicians in 2014. Prior to 2008, only 10% of hospitals had adopted a basic EHR system. But by 2017 the number of hospitals with a certified EHR increased to 96%, and 86% of office-based physicians had adopted an EHR of some kind.
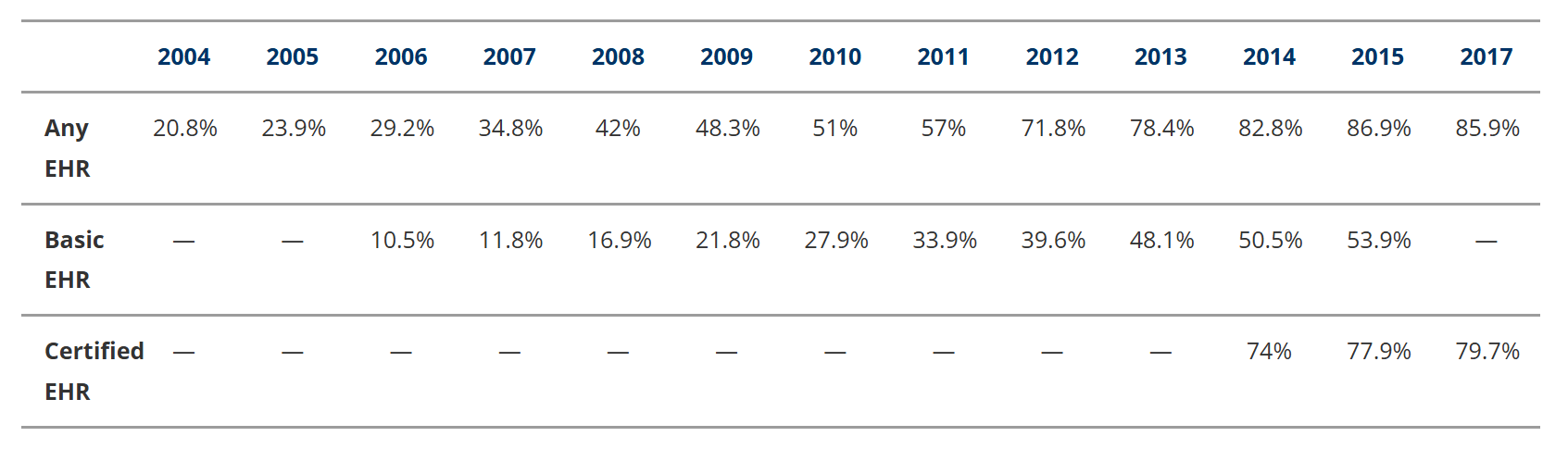
Table 1. Percentage of office-based physicians using EHR/EMR, 2004–2017. Source: Office of the National Coordinator for Health IT, Office-based Physician Electronic Health Record Adoption (Health IT Quick-Stat #50), Jan 2019. https://www.healthit.gov/data/quickstats/office-based-physician-electronic-health-record-adoption
Why do medical practices have to convert EMR and EHR systems?
Changes in legislation, technology, and mergers and acquisitions all drive digital record conversion. From the beginning of healthcare regulation with ERISA to Obamacare, a central theme in healthcare reform has been the cost of bad administrative systems. Miscoding, for example, is one of the most common reasons why insurance companies deny legitimate claims. For this reason, both the government and private sector have invested considerable resources into EMR and EHR conversions. The government expects this program to save costs as well as lives.
But there’s also a more elusive promise: that by creating innovative databases and using artificial intelligence, we can solve some of the world’s most intractable health problems.
At the more practical level of logistics, much preparatory work is required to guarantee smooth conversion of electronic patient records. Technical setup demands include
Data mapping
Extraction and analysis
Machine learning and artificial intelligence
The need for new software and training
But beyond these are eternal challenges in record keeping going back to the origins of medical science.
A brief history of medical records
For almost five thousand years, doctors have tracked medical records by hand. In the evolution of medical records from papyrus to electronic tablets, doctors have encountered a few recurrent problems. One of the most universal questions has been on how to structure the records to best make meaning, for example, by medical narrative or by symptom, diagnosis or treatment.
Reviewing the history of the medical records can sharpen the way we look at EMR conversions today and thus improve system design and patient care.
The first documented medical records occurred in the Bronze Age when ancient Egyptians developed one of the earliest medical science cultures. But they also believed deities and spirits caused illness and death.
Ancient Egypt and the birth of case studies
The Egyptian Imhotep is the earliest (circa 3,000-2,500 BCE) known doctor to conclude that disease and death were natural processes rather than divine punishment. (Imhotep practiced medicine and wrote on the subject 1,000 years before Hippocrates, who, more widely known, is considered the Father of Modern Medicine.)
Imhotep probably wrote one of the earliest known medical texts, the Edwin Smith Papyrus. Unlike other medical texts from this era, which often included spells, the Smith Papyrus is remarkably scientific. The text contains almost 100 anatomical terms, extended sections on ophthalmology as well as obstetrics and gynecology, and describes 48 injuries. Each of these injuries has a case history detailing the type of the injury, examination of the patient, diagnosis and prognosis, and treatment.
From the very beginning, medical records were based on narratives describing pathologies and traumas classified by anatomy. Disease pathology and injury diagnosis and treatment are extensions in the growing taxonomy.
This principle extends through the medical system to today, five millennia later, to the International Classification of Diseases (ICD) Diagnosis Codes medical practices and insurance companies across the world use to categorize injuries and illnesses in EHRs.
Greco-Roman empire: the beginning of anatomical science
Greco-Roman civilization also marked the flowering of rational approaches to medical care, emphasizing a healthy lifestyle as preventing illness. Because both cultures had taboos against dissecting human bodies, knowledge of human anatomy was incomplete. So corresponding medical taxonomy and record keeping were imprecise.
But surgeons like Galen, who treated wounded gladiators, wrote texts on anatomy exposed during injury. Galen served three Roman emperors, including Marcus Aurelius, and lived to age 87. Galen’s influence extended through the Middle Ages. Although his influence was immense, he got much of human anatomy wrong because he based it on dissections of other mammals.
The first known scientific dissection of the human body was performed in the third century BCE in Alexandria by Greek doctors Herophilus and Erasistratus. They founded a school of anatomy and are credited with some of the earliest systemic discoveries of heart valves and neurological function. But they were criticized for conducting vivisections on convicted criminals.
After the Germans conquered Rome in 5 AD, the decline of the Roman empire meant medical advancement was lost through the Middle Ages. Typical approaches to treatment were to consult ancient Greek or Roman medical texts.
The Black Plague forces authorities to consider public health
The Black Plague dominated public health for centuries during the Middle Ages. Among the earliest documented pandemics, the plague swept Europe with two outbreaks punctuating the Middle Ages. The first struck in 542 CE in Eurasia.
The second pandemic began in 1347 and lasted until the late 17th century. The most destructive epidemic in history, it killed an estimated 100 million–almost one quarter of the world’s population. It reduced Europe’s population by 30-50 percent.
The plague forced evolution in approaches to medical records, public health and ultimately urban design. City hospitals kept records of those who died or were infected, and this prompted the first real efforts at public health initiatives with pandemics. City-states with international trade in ports or along the Silk Road developed quarantine policies. Medical records at this point formed the basis of large public health decisions. Infection and death records eventually formed patterns that town planners couldn’t ignore, and they began to realize the importance of clean air, sunlight, water, and burial of waste and human remains. Environmental urban design improved sanitation enough to restore quality of life to that approaching the Graeco-Roman Empire from the previous millennium.
Physicians began rejecting Galen’s theories of the humours and bloodletting and relied instead on empirical methods like observation and trial and error.
Dawn of modern medical records
Modern medical records evolved in the nineteenth century hospitals of large cities like Berlin, Paris, London and New York. In big cities the scale of public health systems encouraged record keeping, both financial and medical, as a way of rationalizing expenditures, diagnosis and treatment. It also provided the infrastructure for teaching hospitals. London’s St Bartholomew’s was founded in 1123 as a teaching hospital, a role it still serves today.
During the first half of the nineteenth century medical records were largely loosely structured narratives of all admissions. At first these were retrospective case notes, written after patient discharge or death.
But by the end of the nineteenth century, real-time recording of case notes and fixed charts replaced retrospective case studies.
By 1911 New York Hospital board suggested arranging case histories by diagnosis, thus creating case studies.
Standardized charts or tables have their usefulness. They allow for cross referencing of similar diagnostics and treatment.
But critics pointed out an over-reliance on this information format destroyed the value of the medical narrative, which provides a richer, more naturalistic and empathetic approach to medicine. Observing and describing symptoms and treatments subsequently drove the evolution of medical data systems. Physicians rely on charts but still value the use of medical narrative.
Flu epidemic and birth of epidemiology
The 1918 flu epidemic revealed huge weaknesses in public health information systems. Public officials lacked the most basic data to monitor pandemic trends and possible public health responses. The Spanish Flu killed between 50-100 million people. The scale of death, disease and data resulting changed medical records forever—and for the better.
“The cornerstone of public health is epidemiology—the study of patterns, causes and effects in disease—and this now received full recognition as a science,” writes science journalist Laura Spinney. “Epidemiology requires data, and the gathering of health data became more systematic. By 1925, for example, all U.S. states were participating in a national disease reporting system, and the early warning apparatus that had been so lamentably lacking in 1918 began to take shape.” (https://www.smithsonianmag.com/history/how-1918-flu-pandemic-revolutionized-public-health-180965025.)
Formalized health informatics first emerged in industrial accident insurance in the 1920s and then second, in health insurance in the 1930s and 1940s.
New networks are often grafted onto pre-existing ones. In the context of the American healthcare system, the electronic health record is based on the needs of insurance companies rather than on patient care and physician workflow.
Paper patient charts were handwritten and kept in files on specially designed shelves until the mid to late twentieth century, when a new technology emerged.
Early computerized medical records designed for insurance not care
One early pioneer of medical records computerization was physician and researcher Lawrence Weed. He proposed a computerized medical record system relying on data collection and curation (Weed, 1968a, p. 595). Weed’s system included standardized interview questions, precision data-collection instruments, and paramedical personnel who enter data collected from patient narratives and physical examinations into standardized electronic forms.
Weed’s central idea was that a computer could then generate a report featuring appropriate data (Weed 1968a, p. 596).
Armed with this report, data curators and management could translate medical records into a set of treatable “problems” for each patient.
These data and their problems have significant implications for both treatment and extra-therapeutic issues. Concerning the latter, Weed was explicit that, “A medical record “will make possible a fiscal management audit” such that managers could measure the use of “resources and services involved in care” directly in relation to the specific problems outlined in the medical record (1968b, p. 657). Weed and his development team took billing and insurance to be of such importance for a complete medical records system that they explicitly recognized the need to “graft” their new records systems onto existing pathways of health insurance data technology.
The team, for example, featured the need to integrate billing into medical records as part of their 1967 seed-funding grant application. Weed, along with lab co-director Jan Schultz and their team, submitted a grant proposal for the development of the computer system embodying Weed’s Problem-Oriented Medical Information System (PROMIS).
The EHR was originally developed for hospitals and universities. But by 1980s market and government forces pushed wider medical systems to digital.
Move from paper to digital, and EMR to EHR
As patient record keeping moved from paper to digital files, two terms have been used interchangeably, though their real meanings differ significantly: electronic medical records (EMR) and electronic health records (EHR).
What’s the difference between an EMR and EHR?
Both an EMR and EHR are digital records of patient health data.
An EMR is a digital version of a patient’s chart. It contains the patient’s medical and treatment history from one practice. Usually, this digital record stays in one medical system and does not get shared with another practice. If a patient switches doctors, his or her EMR remains with the medical system where it originated.
By contrast, an EHR contains more of the patient’s records from other doctors. As such, it provides a more complete and long-term view of a patient’s health. It includes their medical history, test results, history of present illness (HPI), medications, ancillary services, and even demographics and paying history.
An EHR is a longitudinal, all-encompassing record of events and services tied to the patient, including physician to physician referrals. When a primary care physician refers a patient to a specialist, the EHR contains both the treatment provided by the specialist as well as the primary care. A complete EHR contains vast amounts of information including imaging, labs, physical therapy services, dietary restrictions, consultations, medications, down to the disbursement of prescriptions or patient socks.
The personal health record (PHR) contains the information from the EHR but the patient is in charge of the information. They can add and remove information on their own and they decide who has access to the record. The PHR is also an important instrument for in-home monitoring.
“Interoperability” emerges as KPI
Electronic health records started in the 1970s at the Veterans’ Administration. But they didn’t become mandatory until 2014 with the passage of the Patient Protection and Affordable Care Act (PPACA), otherwise known as Obamacare. The push for an electronic health record was to facilitate network of healthcare physicians, devices, pharmacists and institutions that was “interoperable,” that is, could work universally across hardware and software platforms to freely exchange information to enhance patient care. (https://dragonchain.com/blog/blockchain-in-healthcare.)
While the Health Insurance Portability and Accountability Act of 1996 (HIPAA) was passed to set up rules guaranteeing the security and privacy of patient data, Congress passed subsequent legislation to refine patient data regulation.
The federal government has been urging the healthcare industry to switch from paper to digital health files since the George W. Bush administration.
HITECH Act
In 2009 Congress passed the American Recovery and Reinvestment Act (ARRA). Also known as simply the American Recovery Act, this legislation allocated $30 billion to fund healthcare systems to convert to EMRs.
Within the American Recovery Act is a provision for improving healthcare information systems. The Health Information Technology for Economic and Clinical Health Act (HITECH Act) both mandates and funds healthcare organizations to implement the conversion of paper records into EMR.
The reason behind the government’s push towards universal EMRs was to make health records more accurate and accessible to patients and doctors while protecting private health information. It was also predicted to save money in the long run.
The HITECH Act includes incentives to purchase certified EMR systems and create privacy standards. It also authorizes Medicare and Medicaid to provide payments to hospitals and physicians who demonstrate “meaningful use” of electronic health records.
The ultimate goal of this digital revolution in healthcare data is to convert EMRs from different practices into a more comprehensive EHRs that are accessible to patients and approved medical professionals across systems and devices.
Since the EMR Mandate became law, the use of electronic health records (EHR) has increased worldwide. In many ways this has improved patient care, care coordination, and the security of patient information.
EHRs begin replacing EMRs
But the goal of nationwide conversion remains incomplete. And it comes at a big cost. When Partners Healthcare (now Mass General Brigham), a ten-hospital system in Boston, implemented an upgraded EHR system from Epic, they spent $1.6 billion in 2015-2016. When the system launched, it required 1,000 support staff to train new users in the system (Gawande, 2018).
Such transformations have become almost universal. But recent research also indicates the adoption of such comprehensive systems comes with tradeoffs.
EHR systems require maintenance. They also require constant data input from medical devices, labs, doctors, nurses and other clinicians, as well as financial and administrative staff and the patients themselves.
When hospitals undertake electronic health record conversion, at some point clinical staff should compare data in their new EHR systems with that of the legacy system to see what failed to transfer properly.
The importance of electronic medical records to hospital success recalls the old programming truism “Garbage in, garbage out.” In other words, a medical records system is only as good as the quality of its data and how it is stored, mapped and retrieved. Large systems require constant real-time input. In a typical 35 minute appointment, doctors are now spending 19 minutes inputting data into the system. They often spend hours at the end of the day amending their notes. The upshot is today physicians often spend two hours on a computer for every hour with a patient.
While this helps track patient data, it also erodes the connection between doctor and patient necessary for diagnosis and recovery. A few researchers point out the possibility of interaction problems between doctors and patients when using EMRs. Patient eye contact is correlated with higher quality of care. Physicians worry that reducing eye contact with patients to less than half the office visit may make the patient feel the physician distracted, rushed or detached, rather than engaged and empathetic.
Public health research indicates many healthcare professionals strongly dislike the EHR system they use.
When researchers explore the question of why the resistance to EMR and EHR conversion, clinical staff, namely doctors, are a central concern.
Reasons fall along a familiar pattern common to most studies: doctors note their lack of time, their medical system’s lack of adequate financial resources, the high cost of set up and maintenance, and, perhaps most importantly, no clear return on investment (ROI) or proof of improvement in patient care.
Other concerns are more practical: doctors resist because they are worried about their lack of computer skills or desire to perform data entry. They are also less confident in the security of private data, either from identity theft or worse, a hacker staging a DDOS. (Healthcare IT experts this week stressed the need to tighten cybersecurity measures in the wake of Russia launching huge malware attacks on Ukraine, the United States and Europe.)
Software companies, healthcare management, and IT staff design these EHR systems to automate hospital operations and administrative functions. So clinicians generally have little voice in platform development. As a consequence they must adapt their workflow to the requirements and structures of the EHR rather than the system supporting their clinical thought process and workflow.
Most acute-care physicians appreciate that EHRs are worthwhile but feel the system itself is hard to use and distracts from patient care when time is essential.
Some EHR platforms offer the option for clinicians to help them fine-tune the system. As busy as most physicians are, many simply have neither the time nor energy for platform prototype development.
This is where hospital management must step in and invest in staffing requirements, as well as management culture support, to make this possible.
EHR Usability
Usability is about where, when and how clinicians can access and interact with an EHR. Users want that to be anywhere, anytime, and with the fewest clicks, taps, or swipes possible.” (https://www.fortherecordmag.com/archives/JA21p16.shtml.)
Part of the expectation among medical professionals is that if financial apps have become near universal in their “interoperability”—that is, the ability to work with other software and hardware systems–why can’t healthcare data migrate seamlessly from desktop computer to tablet to phone?
The nature of systems is standardization. But really, systems should encourage customization. But even when new platforms designers are in a position to rebuild entire systems from the ground up, they still have to anticipate how future needs could be radically different. Just think of the way smartphone software and hardware development has to anticipate generational changes of moving from 4G to 5G.
Early on in the adoption of EHR standards, researchers raised concerns about clinical staff using a digital system designed for the insurance industry:
“Systems originating primarily as billing systems were not designed to support clinical work flow,” wrote Martin Cowie et al. “Moving forward, EHRs should be designed to optimize diagnosis and clinical care, which will enhance their relevance for clinical research.” (Cowie, Martin R. et al. 2016. “Electronic health records to facilitate clinical research.” Clinical Research in Cardiology. https://link.springer.com/article/10.1007/s00392-016-1025-6.) This is exactly the point behind value-based healthcare systems trying to leverage EHRs into actual patient plans.
How EMR and EHR conversions can go wrong
Bad data maps are a common mistake when starting a conversion. In other words, not having a complete picture of data storage or the data that needs migration leads to multiple system failures.
Some state laws require healthcare systems to keep backups of patient data for years. This can lead to legacy data getting lost in silos. For this reason it’s imperative you review the data to verify that the content of each data field matches its label.
Failing to upgrade the network. Data transition requires bandwidth for upgrades, and this is often overlooked.
Reluctance to adopt cloud storage misses many benefits.
Failure to anticipate workflow disruption. Avoid this by migrating data at night.
Moving healthcare data without conversion experts creates huge risk. Patient records can go missing that are crucial for diagnosis as well as collecting insurance claims. That’s why medical systems should contact our company, ERISA Recovery. We are electronic medical record conversions specialists. We’ve been in the business for over a decade. As a result, we’ve pioneered many machine learning and data abstraction techniques are competitors are still struggling to learn.
Book a free consultation or request a demo of our data migration solutions today.
Tips for Making EMR and EHR Conversions Successful
Establish good communications with staff about the EHR system.
This is an organizational commitment that will affect the lives of all staff and patients. Treat all staff as stakeholders. Ask them what the current system does well and where it needs improvement.
Map your data
It helps to draw a picture of the data you have now and how it will be arranged in the new system.
Tailor your EHR to staff workflows.
Securing the staff’s buy-in is crucial for success. Solicit opinions and recommendations from them based on workflow. Customizing the EHR platform is crucial to making sure the EHR will work for everyone. Many EHR systems like Epic say they encourage customization input from physicians.
Be proactive: Identify ways the EHR could fail in order to prevent problems in the future.
Solicit input from stakeholders to pinpoint ways the EHR could fail and the worst consequences. How could the patient appointment system break down? What about medication alerts? What is the backup plan during transition? Use their input to define what key performance indicators would make the EHR conversion a success.
Consider the needs of your data storage and retrieval, and plan for them to increase.
Allow enough time to train staff
Train your staff for every step of the process. Management must be realistic about the number of hours doctors, nurses and other clinical staff require to learn the new system, in addition to their standard responsibility.
Plan accordingly and reduce staff responsibilities during training to accommodate the extra work.
Start with short training sessions. Beginning with the basics is important. Follow up with practical, planned training that follows typical tasks during the day.
In EHR implementation, practices and hospitals have different needs, just as ambulatory clinics have different needs from acute-care facilities.
Eliminate duplication.
Redundant data entry must be minimized. Patient demographics, for example, need to be input whenever the patient enters the system. But this information also needs to be available throughout all modules and interfaces. Studies of clinicians views of EHRs are similar to most people’s of app designs: the fewer the clicks, the better.
Preserve the legacy system.
Plans for data migration must include preservation of the legacy system. The first reason is to double-check for quality control. And second, as a fallback in case the EHR system has unforeseen failure.
Work with vendors who have extensive EHR implementation experience.
Ask for industry references and meet with former and present clients. EHR conversion is one of the most important infrastructure investments medical practices ever make.
Why choose ERISA Recovery
At ERISA Recovery, we have over 12 years of experience pioneering machine learning, data mining and artificial intelligence in medical finance. If you have any questions about protecting your healthcare organization during electronic medical record conversion, contact us for a free consultation.
* * *
Notes
Charon, Rita. The Patient-Physician Relationship. October 17, 2001. Narrative Medicine: A Model for Empathy, Reflection, Profession, and Trust. JAMA. 2001;286(15):1897-1902. doi:10.1001/jama.286.15.1897
Koopman, Colin et al. BioSocieties. https://doi.org/10.1057/s41292-021-00249-1 . For the Critical Genealogies Collaboratory Accepted: 20 August 2021.
Cowie, Martin R. et al. 2016. “Electronic health records to facilitate clinical research.” Clinical Research in Cardiology. https://link.springer.com/article/10.1007/s00392-016-1025-6.)
Gawande A. Annals of medicine: “Why doctors hate their computers.” The New Yorker magazine. March 28, 2019. https://www.newyorker.com/magazine/2018/11/12/why-doctors-hate-their-computers.
Graber, Mark L. MD, FACP*; Siegal, Dana RN, CPHRM†; Riah, Heather MBA et al. “Electronic Health Record–Related Events in Medical Malpractice Claims.” Journal of Patient Safety June 2019 – Volume 15 – Issue 2 – p 77-85
Siegler, Eugenia L. (2010). “The Evolving Medical Record.” Annals of Internal Medicine, 153(10), 671–.doi:10.7326/0003-4819-153-10-201011160-00012
Spinney, Laura. “How the 1918 Flu Pandemic Revolutionized Public Health. Mass death changed how we think about illness, and government’s role in treating it.” Zócalo Public Square, Smithsonian Magazine, September 27, 2017. https://www.smithsonianmag.com/history/how-1918-flu-pandemic-revolutionized-public-health-180965025.